

1st Degree
Atrioventricular (or AV) heart blocks are usually caused by a delayed, absent, or inconsistent electrical conduction pathway through the AV node. These AV blocks are described as a first degree, having a prolonged PR interval beyond .20 seconds.
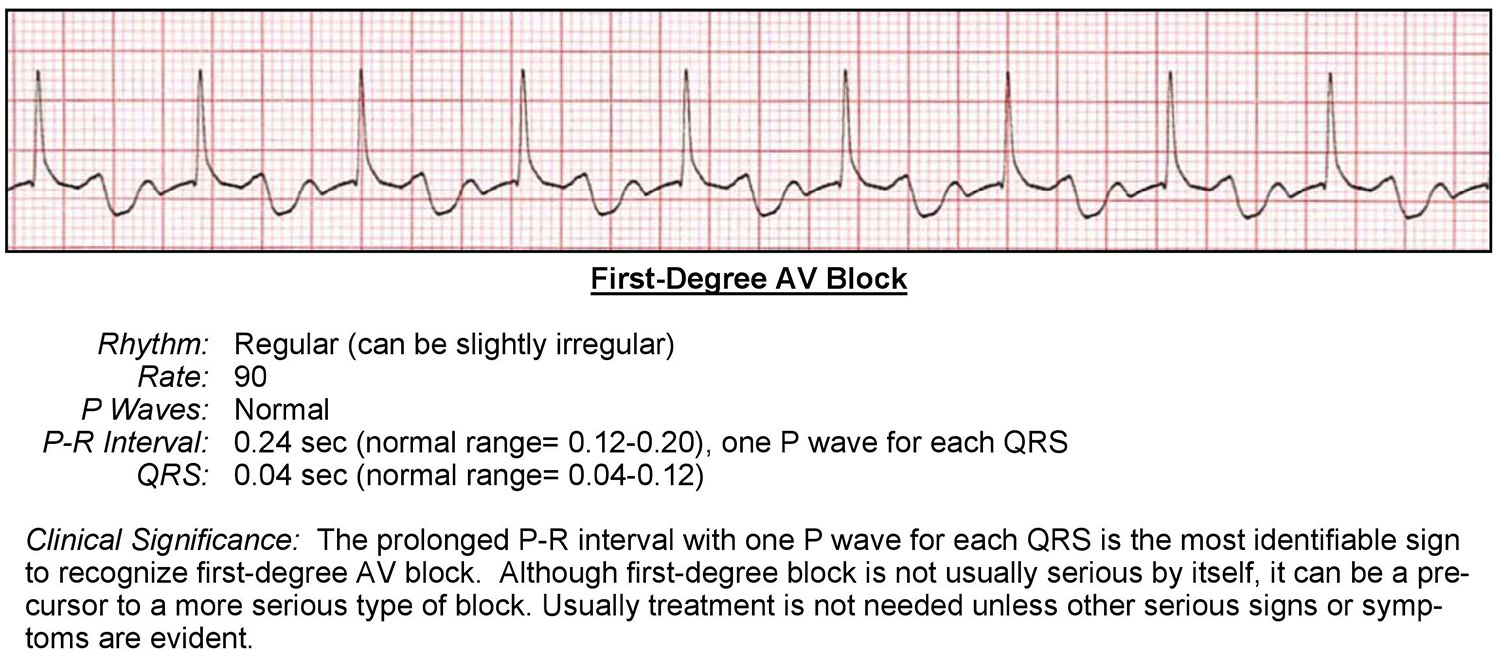

An ECG will show the following:
- Rhythm is regular with a normal or slow rate
- P waves are present and upright
- PR interval greater than .20 seconds
- QRS complex is between .06 and .11 seconds
- P wave to QRS ratio is 1 to 1
There is usually a minimal clinical significance with this form of heart block.
2nd Degree Type 1 (Wenckebach)
A second degree, also called a Mobitz Type 1 block, usually has a progressively widening PR interval. This is followed by a QRS complex that is progressively delayed at the AV node until completely absent. It then only shows a P wave without a QRS following it.
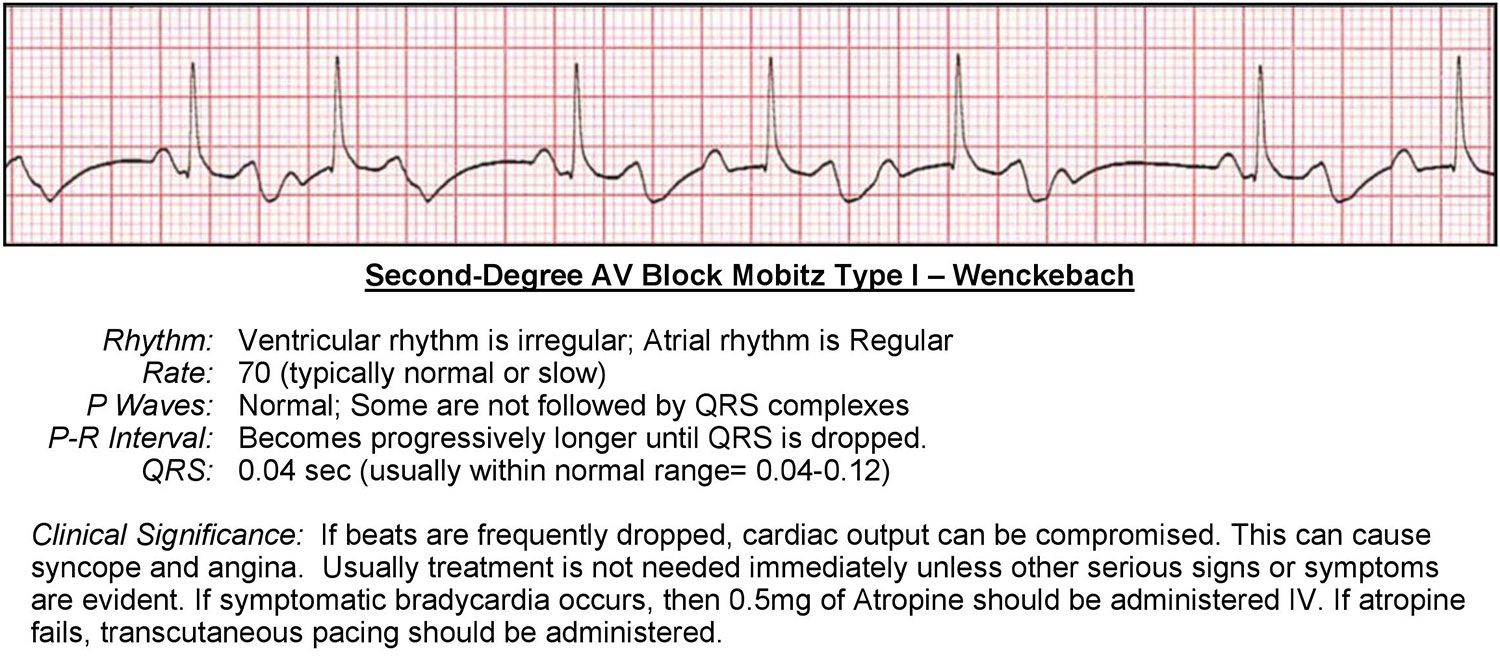

An ECG will show the following:
- Rhythm is regularly-irregular
- Rate is normal or slow
- P waves are present and upright
- PR interval is progressively lengthening until a QRS complex is dropped altogether
- QRS complex is between .06 and .11 seconds
- P wave to QRS ratio is 1:1 until a P wave is blocked
This is commonly caused by a heart disease affecting the AV node or by vagal stimulation, which is often associated with:
- Difficult bowel movement
- Coughing fits
- Medications
2nd Degree Type 2 (Mobitz)
The third type is called Second Degree Mobitz Type 2 and usually occurs when the heart block is below the AV node.
Usually the ECG appears to have intermittent blocks where some P waves do not have QRS complexes following. There is no elongation of the PR interval. In the case of this Type 2 heart block, the rhythm is variable depending on the P to QRS ratio.
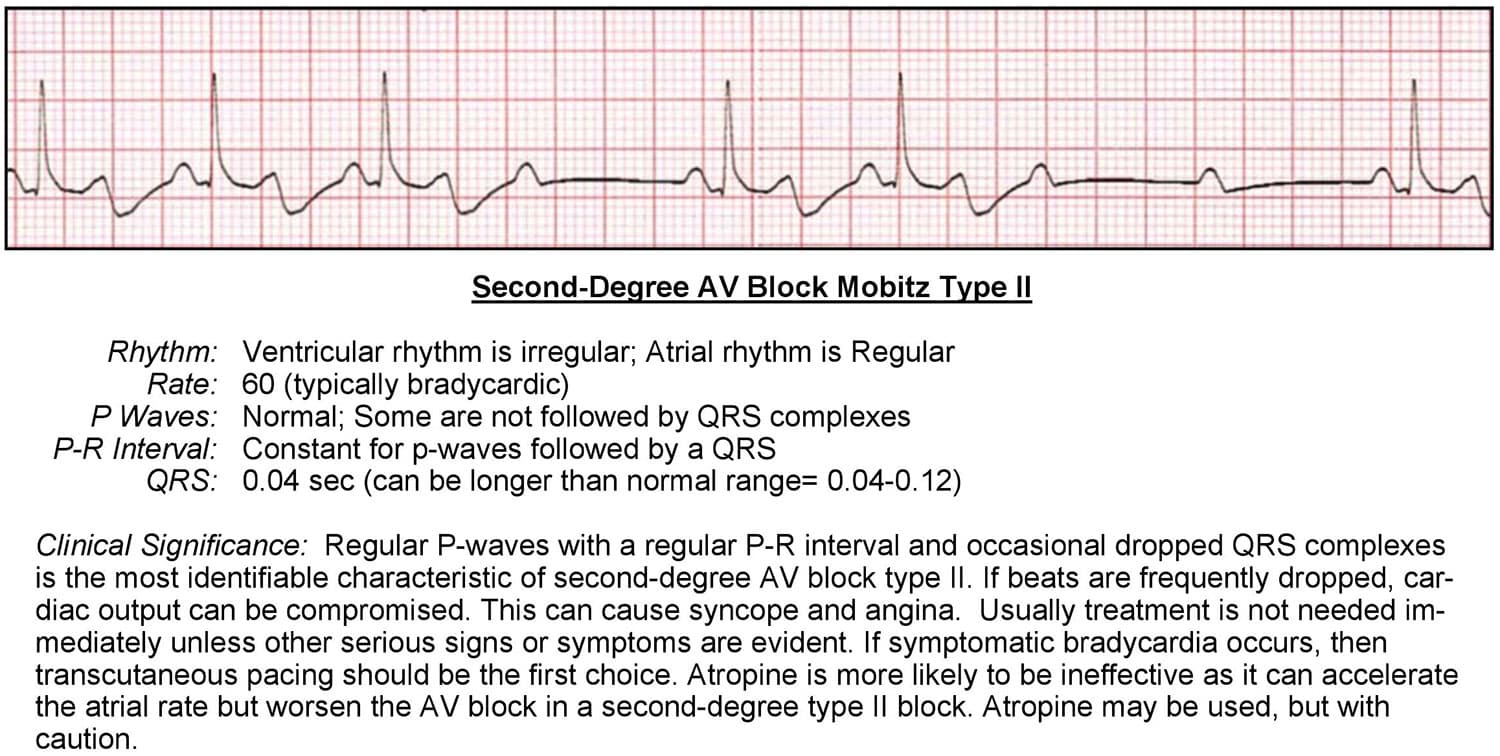

An ECG will show the following:
- Rate is variable but will usually be slow
- P waves are present and upright
- PR interval will be between .12 – .20 seconds of the normally conducted complexes
- QRS complex is .06-.11 seconds
- P wave to QRS is variable and can be seen as 2:1, 3:1 or even as much as 4:1 and beyond.
This Type 2 heart block is usually from a more advanced and severe heart disease. It can originate from damage below the bundle of His. Because of this, Mobitz Type 2 can deteriorate more quickly into a symptomatic dysrhythmia and even become a third degree heart block.
3rd Degree Complete Block
Lastly, the third degree complete AV heart block occurs when electrical conduction is completely blocked between the atria and ventricles. The exact location of the block can vary but is usually somewhere around the AV node or lower. It will disassociate the SA pacemaker from the AV or bundle of His pacemakers, creating an ECG with regular P waves and regular QRS waves. But these waves will be at different rates and completely disassociated.
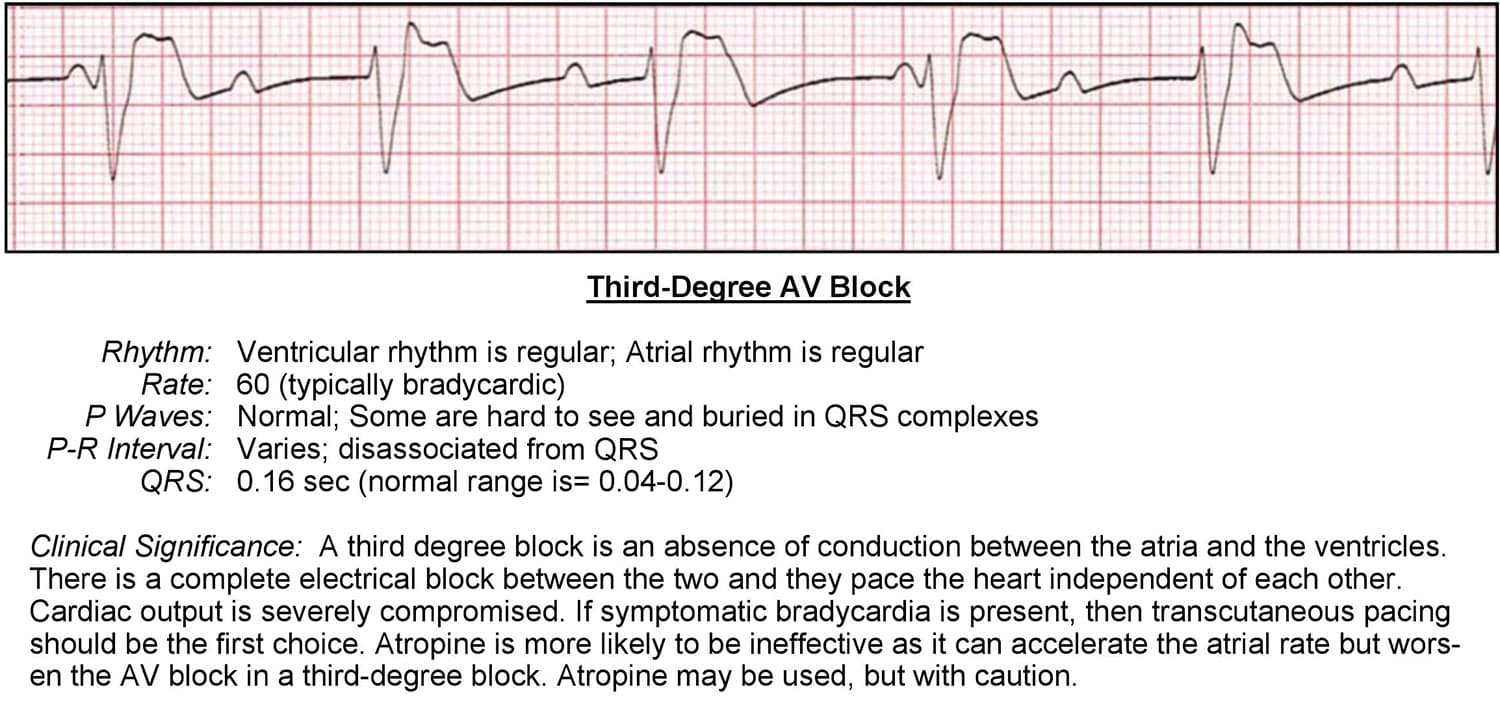

An ECG will show the following:
- Rhythm is regular
- Rate is bradycardic between 20-40 beats per minute
- P waves are present and upright
- PR interval is variable with no real pattern
- QRS complex is greater than .11 seconds
- P wave to QRS ratio is variable
The clinical significance of this dysrhythmia is serious. The patient will usually be symptomatic and unstable due to the very slow bradycardic rhythm.
Remember, the block is stopping any pace that would originate from the SA node, so the ventricular pacemaker will stimulate a pulse rate of closer to 20-40 beats per minute. This is usually not enough to keep a stable blood pressure. This is why the ECG will usually have wide QRS complexes.
Studies have shown that third degree heart blocks may be transient or permanent depending on the underlying cause.